
Three bones theory and the sensory stations of the deep core:
An anatomical description of evolutionary mismatch and sitting disease as kinesthetic dystonia.
A summary statement.
Three bones theory states that there are three major bones, each located at the heart of a major juncture of the body, and these bones are atrophied, forgotten and weak, or are actually distorted. These bones are located on our central axis, or what is called the deep core. Each bone is located at the center of a major juncture of our body and is essential to our structural balance. The areas where these bones are located are also our most sensitive and protected areas, full of physical, neurological, chemical and circulatory inputs: they are sensory stations of the deep core. Their loss results in the collapse of our structure, chronic pain, and a loss of bodily self-awareness with significant mental and social-emotional consequences. This is a result of immobilization and the evolutionary mismatch our bodies deal with in modernity.
The Three Bones
The three bones are the jaw (mandible), pubic bone (pubis), and big toe (hallux).
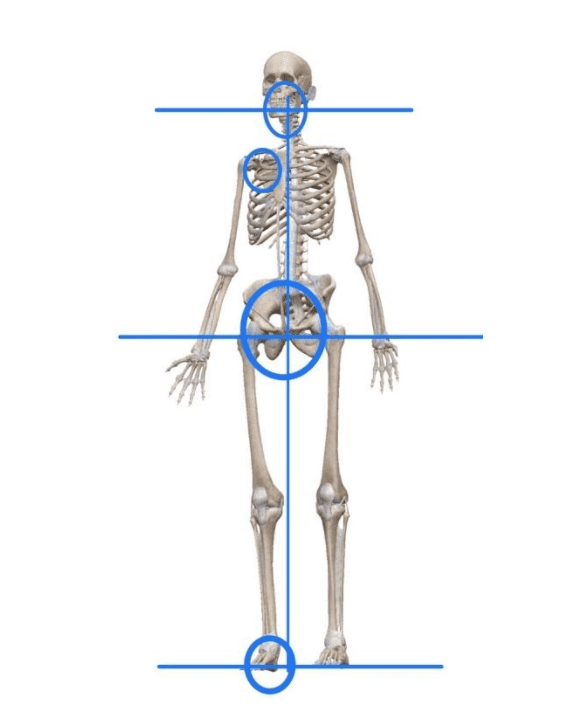
Three bones theory states that three major bones are missing, atrophied, or distorted at the center of the major junctures in the body. These junctures are complex but easily identifiable. They are each on the midline of the front of the body, at each end of the spine as well as the feet, where we connect to the ground. Each bone is the largest and most prominent bone in its area: the jaw, the pubic bone, and big toe. A fourth bone, the scapula, connects the heavy extremity of the arm to the back of the rib cage and in so doing forms the armpit.
Removing these major, central bones from active engagement and function is like pulling the linchpins out of a machine. The structure collapses. Three Bones Theory describes the way our structure is compromised at each consecutive juncture and this happens in a process we are not aware of and by which we gradually lose self-awareness. The compensating posture of sustained collapse that we resort to becomes the new normal. Three bones theory describes this in terms of kinesthetic dystonia.
Removing these major, central bones from active engagement and function is like pulling the linchpins out of a machine.
These important but lost or missing bones are the jaw, pubic bone, and big toe. The jaw is located at the neck, where the head meets the spine. It is atrophied by our soft diet resulting in malocclusion of the teeth and airway obstruction (Kahn and Ehrlich 2020). A slack and atrophied jaw results in collapse of the anterior neck and compensatory tension at the back of the neck.
The pubic bone, located in the groin where the legs attach to the body, is the structure that balances the low back. The low front balances the low back, but this area often has low tone and suffers most directly from the effects of prolonged sitting. The area also is rendered inert due to shaming and trauma. Not only pelvic imbalance and low back pain, but a reduction in core strength are the result of the loss of this area. We complain about low back tension but we fail to notice that the balancing structure of the low front, or groin, is weak and offline. It has been called psoas insufficiency syndrome (Bachrach 1998).
The sensory station of the feet are where the body meets the earth and the big toe, at the center of this area, is our most important adaptation from the primate foot (Holowka and Lieberman 2018). The primate foot had an opposable big toe, but our straight big toe and rigid arch is a crucial mechanical part of our ability to stand on two feet, walk and run. In modern shoes this crucial structural element becomes distorted, and this results in poor grounding, the atrophy of the arch of the foot, and contributes to the further collapse of our structure upstream.
A fourth missing bone is the scapula.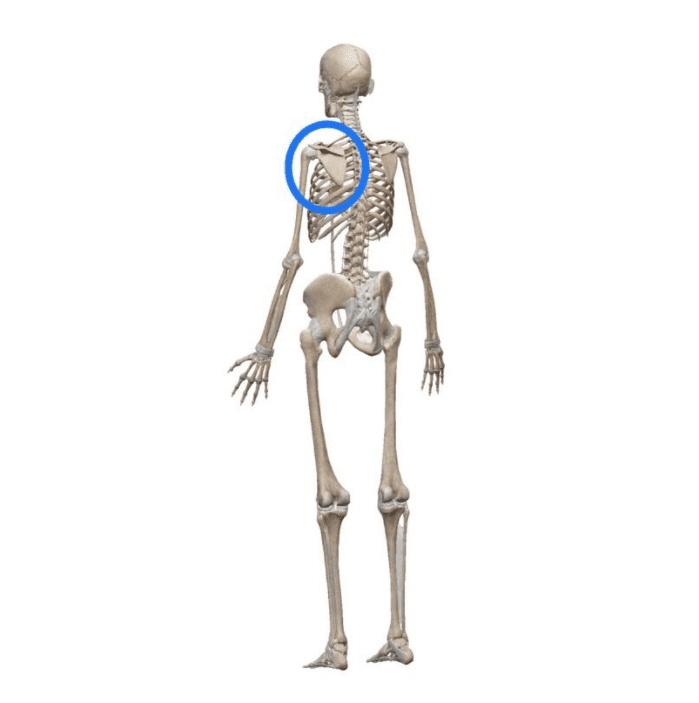
A fourth and major missing bone is the scapula, which anchors the arm to the body on the back of the rib cage. While not directly on the central axis, it plays a major role in our structural balance and its malfunction, called scapular dyskinesis, results in a heavy burden on the neck and head (Kibler 2013). The scapula is clearly the largest and dominant bone of the area but has been forgotten and down-toned as a result of trying to organize the arm around the shoulder and neck. The structural imbalance that results is called the slouch.
The Sensory Stations
The sensory stations of the deep core: groin, throat, armpit, and feet.
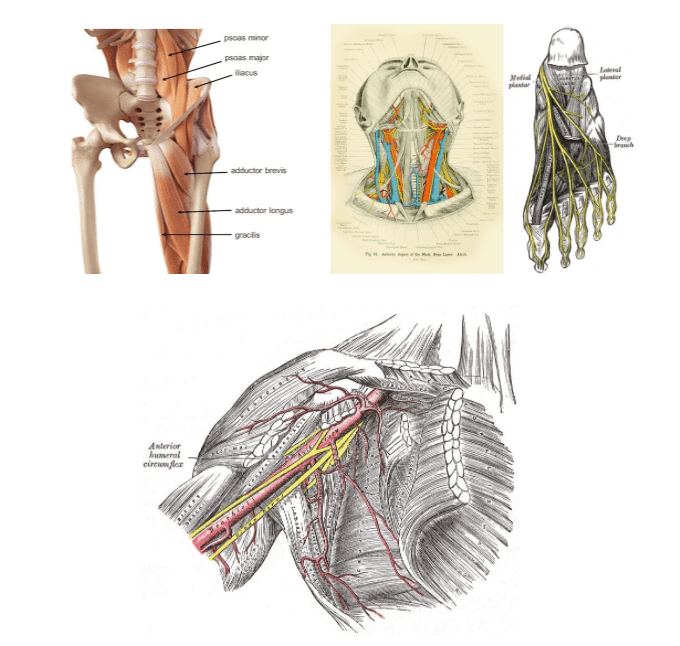
Because each bone is located at a major biomechanical and physiological juncture of our body, the area it is the center of is also exceptionally sensitive. We are designed to feel and know ourselves in these areas. These are sensory stations of the deep core and are designed to allow us to feel ourselves on a profound level, both consciously and unconsciously. Loss of these areas means we have lost touch with important parts of ourselves. However, we can also use this knowledge to redirect our attention and inner awareness, to increase activity, tone, and to initiate deep personal healing.
The sensory stations are located in the parts of our bodies where we fold up into the fetal position. These are our most complex, sensitive, and most protected areas. In these areas we have delicate skin and hair and this is where we are designed to touch ourselves, boosting proprioception, or positional awareness. The sensory stations naturally attract attention to themselves, and structurally they are the best focus for our motor control. The sensory stations are where we are “in touch” with ourselves, others, and the earth. “The feet feel the feet when they feel the ground” explains Mrs Who. Our feet are among our most complex and sensitive body parts. The feet must be able to organize and balance the structure above them. Our feet are very specifically designed to do this for our unique upright posture. They are far more complex, dynamic and sensitive than those of four-legged animals. The human foot is a uniquely complex biomechanical sensory station designed to let us live and work and run on two feet on the earth. We should not be dismissive of them or of any of the important bones and sensory stations of our body.
Like the navels of an orange the deep core must emerge at either end of the spine and it does so in a blossom of sensory apparatus. This is easy to see in the groin and the throat. In the throat we can include delicate organs of expression and speech, breathing, digestion, lymphatics and of course muscle. These are also centers of physical activity and movement. The sensory stations are full of fans of muscles that radiate outward and have the effect of pulling us together. This is where we “get it together.” We “get a grip” in these structures.
These stations are where we get in touch with ourselves. The pubic bone in the groin, for example, is where we bring our legs together, in adduction.
Although these are centers of activity and sensation, our maladaptive response is that they tend to be neglected in favor of their much less sensitive but larger and more prominent structural opposites. We have to choose more wisely where we decide to focus our attention. The low back receives a lot more attention than the groin, for example, as we struggle to maintain our imbalanced system, stabilizing single-handedly with the extensors and lateral rotators of the low back. But the low back is much less sensitive and offers much poorer motor control options than the groin. It is common to direct attention to the hips to balance the low back: “hinge at the hips”, we are told. This is mechanically correct, but it is the groin that is designed to manage this process. Three bones theory proposes that we remember that the low back is not opposed by the hips but by the groin. By returning awareness to the groin we can restore healthy lumbopelvic rhythm.
The same has already been shown to be true for the shoulder (Kibler 2013). The shoulder, the opposite of the armpit, is like the low back; it is relatively insensitive and offers a poor focus for motor control. It is not clear whether the modern word shoulder derived from the ancient Germanic term for shield, but it certainly functions well as one. Try as we might focusing on the shoulder and neck is a very poor way to organize the arm. It is just a very poor choice biomechanically speaking. In contrast, it is the sensory station of the armpit where we need to direct our active attention to restore good scapulohumeral rhythm. The shoulder has gotten overwhelming attention by surgeons as well as in the public mind. We all struggle with “shoulder pain” but it is a misdirected diagnosis. Scholars have admitted that they have neglected to study of the scapula until recently. No one has thought to identify the armpit as the anchor of the arm and most powerful link in the arm’s kinetic chain of movement. The humble human armpit fits the job description and actually works wonders when given a chance.
The jaw and anterior neck tends to be slack in modern contexts. In contrast we commonly experience tension in the opposite area, the back of the neck. Instead of holding our self in this sort of compensatory pinch at the back of the neck we want to increase our awareness in the jaw and the throat. A gentle smile is a big help to turn this balancing structure on.
Understanding these bones and the sensory stations they are at the heart of gives us insight into our structure and how to balance it. In the process we will restore our inner sense and our confident sense of self. We are designed to collapse in these areas but we are also designed to restore and maintain our structural balance here as well.
The Deep Core
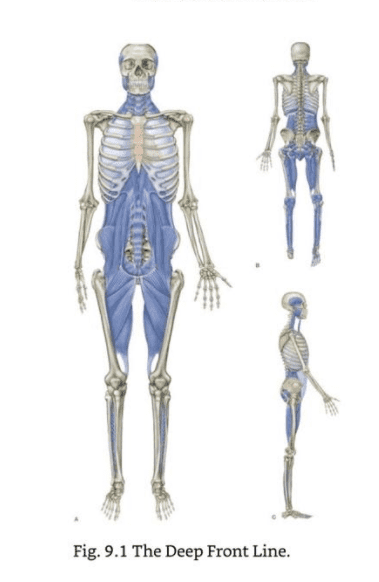
The deep core is “a continual tissue connection from the toes via the psoas to the tongue” (Myers 2014). The deep core consists of all of the muscles in our deepest self and runs up along the front of the spine, including the psoas, the diaphragm, the muscular sheath around the heart called the pericardium, and the anterior neck muscles. It is essential to posture, movement, and our stability. It underlies and supports all of our movements but is not merely mechanical. The deep front line is involved in the “general core collapse which accompanies depression” (Myers 2014) and, from the perspective of somatic psychology, this deep myofascial continuity is where trauma is held. Three bones theory is an attempt to unpack the deep core and understand it in the context of the world we live in.
Sitting Disease and Evolutionary Mismatch
Sedentarism, also known as sitting disease or more formally, the global physical inactivity pandemic (Kohl 2012), is a major cultural cause of this collapse. The mechanical implications of our soft, processed food diet and the effect of bad footwear are also a part of the problem. Modern industrial society has not been kind to the human body. We can think of this from many different perspectives but if we consider this problem in terms of our musculoskeletal system we can approach it with clarity, intention, and from within ourselves.
Three bones theory is an anatomical approach to what is called the “Great Mismatch” (Ehrlich 2018). Evolutionary mismatch is a term from biology that refers to the inability of our bodies to adapt to the environment we have created for ourselves. Three bones theory explains this maladaptation in terms of our muscles and bones, our most tangible and volitional system, in the hopes that we can become more self aware and take a natural, easy, and active approach to the problem. Three Bones Theory attempts to describe the problem of our body’s maladaptive response to modern life in terms of muscles and bones because these are our most easily controlled and easily felt tissues.
Somatic Trauma
There is a general design tendency within modernity towards immobilization. This often takes the form of a requirement to sit still with an implicit threat as a result of failure. This threat can be embarrassment, disapproval in school, or discipline in the workplace. Prolonged siting is both a leisure activity and a forced behavior. There are many moments when sitting is not in your own best interest. This is subtle social control through mandatory and habitual immobilization of the body. Immobilization together with fear produces trauma and this is held in the body. The modern body shows every sign of having been rendered immobile and flaccid as a result of trauma.
“Flaccid muscles,” Levine explains, “belie how the body collapses” in the fear response (2010). Fear often results in immobilization, or “playing dead.” This can be dramatic, as in feinting and passing out, or it can be subtle, developmental and chronic, accumulating over time. Of course we understand that trauma results from extreme experiences of fear, but we also understand now that persistent and subtle repression can result in significant trauma as the effects accumulate over time. It is especially this subtle and persistent trauma that we must understand and learn to correct. We “can learn to bring life back into those muscles as the fragile fibers learn to fire coherently and thus vitalize the organism (Levine 2010). Three bones theory is an effort to describe in simple anatomical terms the body’s response to social and developmental trauma.
Kinesthetic Dystonia
Three bones theory seeks to explain sitting disease as a form of kinesthetic dystonia, the loss of sensorimotor function. The key goal is not just a restoration of muscle tone and function but a recovery of our inner sense. To restore this lost tone we must also restore kinesthetic awareness. We must be “mindful of how [our] muscles feel from the inside” (Levine 2010). The deep core expresses itself in these key bones, each at the heart of fans of muscles, within rich and tender sensory stations. Of course there is a lot more going on than movement sensors in these areas, but movement is a very good practical focus and will bring everything else along with it nicely. A lack of movement and lack of understanding of how to move in an integrated way is the problem that three bones theory seeks to address. Good posture is not the goal. Posture is simply the starting point for movement. Movement is the goal.
It is most useful if the name we give to this condition includes within it the solution, and not just the problem. Kinesthesia means awareness through movement. It is the inner sense of the body and it is related to awareness of our own structure, our muscles and bones, and our movement. “Dystonia is a disorder characterized by involuntary muscle contractions that cause slow repetitive movements or abnormal postures” (NINDS 2021). Dystonia means faulty muscle tone or, in other words, spasms. These spasms can be shaky or rigid or postural and the condition is usually considered to be neurological and rare. The most common form of dystonias are idiopathic, meaning there is no identifiable neurological cause. Kinesthetic dystonia, however, is postural and is far from rare. Instead, it has become a global pandemic due to our sedentary lifestyle. Kinesthetic dystonia tells us we have basic problems in the postural system involving a loss of tone and movement awareness. Three bones theory explains the etiology of this condition in anatomical terms and points you toward just a few specific, easily identifiable parts of yourself as the most likely answer.
The inclusion of our own subjective and conscious, active awareness in the healing process is a crucial ingredient in the label of kinesthetic dystonia. Three bones theory explains how our collapse is a body wide, structural process and restoration of function to that system is something that we are designed to do naturally and successfully in the course of everyday life. We do this by understanding how our structure integrates and fits together as an experiential whole. The simple architecture of the three bones, their sensory stations, and the context of the deep core tells us how to actively balance ourselves despite a variety of physical, psychological, and environmental stressors. We do this by returning attention to these missing bones and to our central sensory stations. Our task begins with restoring bodily self awareness and Three Bones Theory is your guide to this process.
References and Notes
Bachrach, R., Micelotta J., & Winuk C., (2007) The Relationship of Low Back Pain to PSOAS Insufficiency, Journal of Orthopaedic Medicine, 29:3
Earls, J., (2021). Understanding the Human Foot: An Illustrated Guide to Form and Function for Practitioners. North Atlantic Books
Ehrlich, P., Blumstein, D., (2018). The Great Mismatch, BioScience, Volume 68, Issue 11, November 2018, Pages 844–846.
Kahn, S., Ehrlich, P., Feldman, M., Sapolsky, R., & Wong, S. (2020). The Jaw Epidemic: Recognition, Origins, Cures, and Prevention. Bioscience, 70(9), 759–771.
Kibler WB, Ludewig PM, McClure PW, et al (2013). Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the ‘scapular summit’. British Journal of Sports Medicine, 47:877-885.
Kohl, Harold & Craig, Cora & Lambert, Estelle & Inoue, Shigeru & Alkandari, Jasem & Leetongin, Grit & Kahlmeier, Sonja. (2012). The Pandemic of Physical Inactivity: Global Action for Public Health. Lancet. 380. 294-305. 10.1016/S0140-6736(12)60898-8.
Holowka, Nicholas & Lieberman, Daniel. (2018). Rethinking the evolution of the human foot: Insights from experimental research. The Journal of Experimental Biology. 221.
Levine, P., (2010). In an Unspoken Voice, North Atlantic Books.
Myers, T. (2014) Anatomy Trains: Myofascial Meridians for Manual Therapists and Movement Professionals. Elsevier.
National Institute of Neurological Disorders and Stroke (NINDS), Dystonias Fact Sheet. https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Dystonias-Fact-Sheet accessed 12.29.21