
The hips. Peaches. The area where your femur, the longest bone in your body, rests neatly into a concave structure that looks like a cup and is actually the meeting place of the three bones that make up one half of your pelvis. (Fun fact: your pelvis is made up of two halves. Each half contains three bones, the ilium, the ischium, and the pubis. The place where they join together is the acetabulum, aka as the hip joint.)
The exact location of the hips varies based on whom you are talking to. Many people think of their hips as the lateral gluteal area. While these muscles all function to cause movement and disperse load at and across the hip joint, the actual hip joint is located more anteriorly on the pelvis, below the iliac crest.
While the hip joint is stable due to the depth of the acetabulum, there are a number of muscles and ligaments that work to maintain the stability and triplanar movement at the hip joint. (All joints are actually tri-planar in nature. The act of walking requires slight rotation to accommodate force and propel us forward.) The 21 muscles that at the hip allow the femur to move; they also allow the pelvis and trunk to move over the femur (). Coordinated movement at the trunk, pelvis, and lower extremity create a sense of mobility and stability at the joint—when you use the body in a dynamic, varied way, joints thrive. Sensations of tightness, instability, or weakness can often be traced by to a general lack of strength and mobility throughout the trunk, pelvis, and leg.
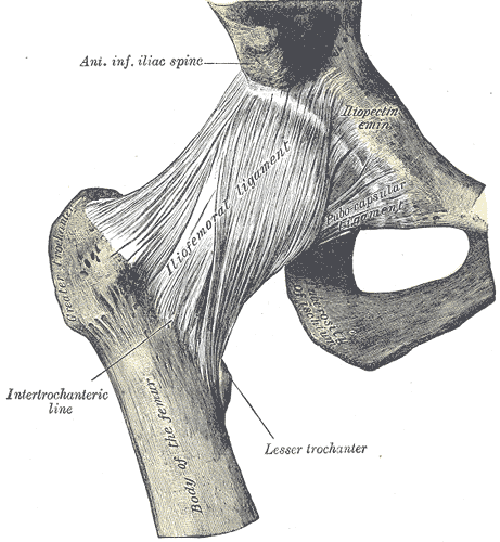
One of the ligaments that supports the front of the hip joint is the iliofemoral ligament. This ligament is shaped like a Y and is conveniently referred to as the “Y ligament of Bigelow.” It is extremely strong and thick, providing stability to the joint. (Ilio refers to the ilium and femoral refers to the femur, which tells you the ligament connects the ilium to the femur). There are other ligaments, like the pubefemoral ligament and the ischiofemoral ligament, that reinforce stability throughout the joint.
Stability throughout the joint is also provided by the acetabular labrum, and blood supply is provided primarily by the femoral artery. There are three different nerves that innervate the hip (the femoral, obturator, and superior gluteal). The hip is a sensory rich area that generates power, integrates with the lower extremity and torso, and connects the lower extremity to the pelvis. How the hip moves depends on how the pelvis moves and how the foot moves, which means when you are assessing hip function, you should also assess pelvis function and foot function.
Since we are asymmetrical on many levels, from our anatomy to our habits and behaviors, it’s not uncommon for the two sides of the pelvis, the two hips, and the two legs to function differently from one another. Just about everyone who begins a new movement hobby will experience this at some point. Balance is often easier on one leg, and one hip tends to feel more mobile than the other, or maybe rotation is easier on one side versus the other.
Movement performed as an athletic skill or hobby generally takes advantage of the multi-planar ability of the hip and pelvis. This is in direct juxtaposition to the to many of the traditional strength movements performed in the gym, which are done done in a symmetrical fashion or cued in a symmetrical way. These more traditional movements, like squats and deadlift, can be a great way to build strength and reinforce a sense of center; however, they don’t expose the lower extremity to the wide range of dynamic mobility necessary to change directions while running, throw a ball, or vault over an apparatus.
Asking individuals to perform movements that require both open and closed chain hip mobility in a variety of ways does more than just prepare people for feats of athleticism. Two of the more common hip complaints seen in a general population setting are FAI and greater trochanteric pain syndrome. As you will see in a moment, both of these (conditions? Issues? Diagnoses?) benefit from multi-directional strength and mobility that can be accessed both subtly and more overtly through dynamic movement exercises.
FAI, aka femoacetabular impingement syndrome, is a clinical diagnosis that refers to a cluster of symptoms related to abnormal morphology of the hip socket, head of the femur, or both (). The theory is the altered anatomy leads to a change in efficient loading at the hip joint, increasing an individual’s risk for labrum injuries or degeneration to the surface of the hip joint.
If you have been diagnosed with FAI, before you panic because the above information sounds terrible (which is consistent with reading reviews in medical journals—it tends to sounds far more dire than it actually is), consider that anatomy is not consistent from person to person. People can have extra vertebrae, scapulae that are shaped differently, and acetabula of varying depths. The idea that our bony anatomy dictates our fate is like suggesting our genes dictate our fate—just like our genes are one of many factors the determine health and behavior, our anatomy is one factor of many that determines our physical expression of movement and how we experience that physical expression of movement.
One of the common complaints with FAI is the sensation of pinching in the anterior portion of the hip joint during flexion, adduction, and internal rotation; curiously (or maybe not so curiously for those of you who study such things), altering pelvis position, down regulating the nervous system, and/or using isometric contractions with the femur in different positions can often immediately alleviate the pinching sensation. Whether or not the effects or permanent depends on whether there are significant degenerative changes to the hip and/or how the person uses their body when they aren’t with you.
*I trained a woman for about six months who was trying a holistic approach to manage the pinching sensation in the front of her left hip. She would always feel better when she left, only to have the pain promptly come back. After about eight weeks of working with me, I began encouraging her to see an orthopedic because even though she was diligent with her homework, the strength wasn’t holding. She finally went, and sure enough, there was significant degeneration in the hip that implicated a hip replacement would likely be the best option for her.
Try this: Come into a standing position. Float your right foot off the floor. Begin reaching from the groin down to the inside of the foot away from the pelvis. Keep reaching the inside of the leg as you begin to reach from the outside of the hip all of the way down to the outside of the foot into the floor. It’s like both the outer leg and the inner leg are reaching away from the pelvis all of the way down to the feet. Hold there for three breaths.
Relax. Compare your legs. Does the pelvis and hip area feel different on the left leg than the right?
Greater trochanteric pain syndrome (GTPS) is a common cause of lateral hip pain, particularly in women between the ages of 40-60 (). The cause of the discomfort was originally attributed to trochanteric bursitis, but imaging studies suggest that GTPS is actually the result of tendinopathy in the gluteus medius and/or minimus; the bursae may or may not contribute to the pain. And, get this: a recent review on this topic in the British Journal of General Practice hypothesizes abnormal hip biomechanics predisposes someone to gluteal tendinopathies, with weak hip abductor muscles adding to the compressive forces on the gluteal tendons.
If you read enough physical therapy journals, you will see terms like “abnormal hip biomechanics” thrown around. This leads the curious reader to ask, “what does normal look like” and “if someone has abnormal hip biomechanics, why didn’t it hurt sooner?”
Physical therapists have lots of ways to measure what “normal” or “adequate” range of motion looks like. It’s usually a passive measurement involving a goniometer and numbers insinuating you should be within a specific range to have normal biomechanics. I am not a physical therapist, and goniometers aren’t terribly interesting to me, so instead I see if the person has adequate range of motion and strength to coordinate movement with the joints above and below the joint in question. If I am looking at the hip, I check coordination with the pelvis and knee (and, per my introduction, the foot). This usually means I end up looking at the thorax and the shoulder as well, because it’s all connected, and if one area isn’t integrating well into movement, usually another area isn’t integrating well into movement. Normal, then, is relative to the individual’s capabilities and anatomy.
It didn’t hurt sooner probably because the person didn’t push it sooner. In my experience, when someone comes in with sudden onset lateral hip pain, it’s because they decided to walk more/stand more/go for a hike for the first time in ten years/crawl around in their attic searching for their high school yearbook for their fortieth high school reunion. The ability to adapt to a wide variety of positions and have the endurance to withstand new activities without experiencing neuromuscular fatigue is dependent upon a baseline of strength, mobility, and endurance. The movement professional’s job is to expose people to a wide variety of positions in a way that feels safe, efficient, and strong; durability (i.e., GTPS prevention), is predicated upon previous movement experience and the ability of the individual to use the lower extremity in a way that is efficient.
Efficiency is based on co-contraction. In the example above where I asked you to reach both the outside and the inside of the leg to the ground, you accessed multiple muscles to stabilize the femur in the hip joint. There are a number of ways to find co-contraction of the hip muscles to stabilize the femoral head, but I will save those for a later post. For now, just know the supported the head of the femur feels in the acetabulum, the more stable the joint will feel and the more the load will be dispersed across a variety of muscles, rather than the load always defaulting to one place.
An important thing to remember when pondering hip mechanics is that the multi-planar movement at the hip is dependent upon the multi-planar movement at the pelvis. I alluded to this earlier, but basically, if the pelvis lacks the ability to move in the sagittal, frontal, or transverse plane, it will be unable to perform the oscillating movement that allows the femur to swing freely in the acetabulum or the pelvis to rotate freely over the femur. Both are important and both should be integrated in a mobility and strengthening program if the goal is to integrate hip joint into dynamic movement.
For an example of what it’s like to incorporate awareness, mobility, and strength at the hip joint, enjoy this 17 minute practice.