

HISTORY and BASICS
Extreme ranges of motion in peoples’ joints have been recognized since Hippocrates, or more likely the Stone Ages when a girl seemed to find it easy to pick fruit while straddling two trees. In more recent history in 1949 the medical community finally coined the more extreme cases of hypermobility as Ehlers-Danlos syndrome(EDS). It was named after two dermatologists who noticed a lot of patients with increased laxity in the skin and joints, combined with other seemingly unrelated but common systemic symptoms.
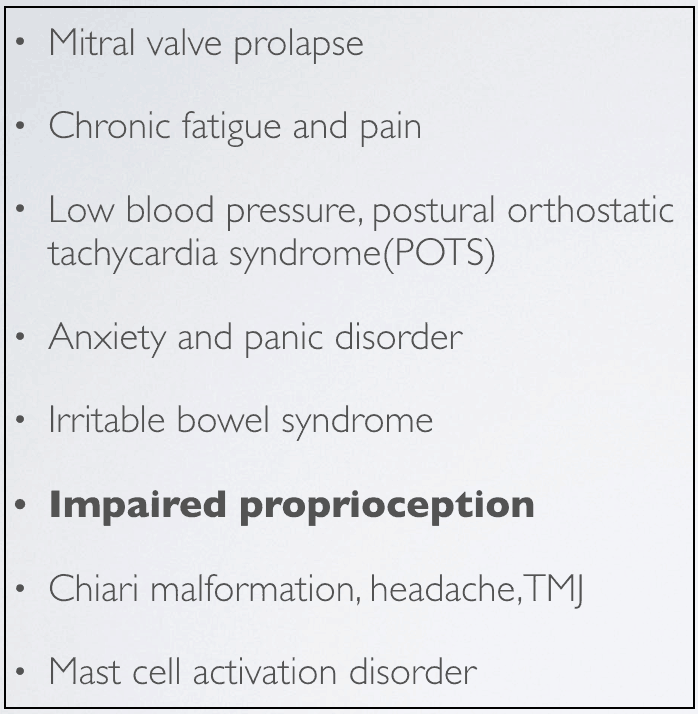
These lesser known symptoms are pictured below. These symptoms are due to the fact that this condition is an inherited connective tissue disorder. The connective tissue effected is collagen which is everywhere in the body, therefore symptoms are widespread and not just limited to joint laxity.
THE SPECTRUM
I talk about hypermobility quite a bit, and am asked a lot of questions on the subject. There are many systems involved, and lots of variability which makes it a complex condition to tackle. Because of this I’ve tried to create an overview of some of the key concepts that can help people understand this condition.
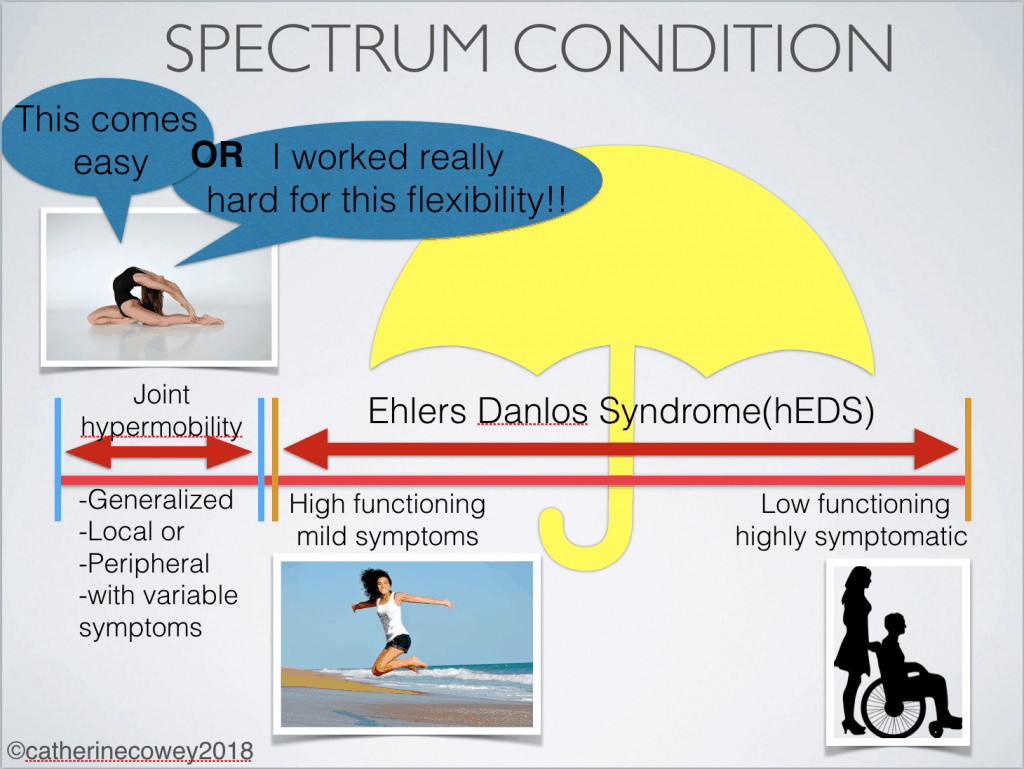
I believe the most important take home when looking at the subject of hypermobility spectrum disorders is the middle term, spectrum. This is illustrated in the picture below that shows the breadth of hypermobility. Using this slide is a good place to start in figuring out the basics of what hypermobility is, and how to go about choosing helpful exercises.
When considering a condition that lies on a spectrum it can be helpful to think of a condition everyone is familiar with, like autism, in which the idea of spectrum is well understood. A question often asked with this diagnosis is, ‘Well, where are they on the spectrum?’. Some autistics are high functioning, needing minimal care, and are possibly heads of large tech companies. While on the other end, people can be highly symptomatic needing a high degree of care.
Hypermobility works in a similar fashion. People can have the same genetic condition but they will present in each individual differently. This is partly due to the fact that an inherited condition like hypermobility interacts differently with each persons’ specific genes creating some of this spectrum effect. The spectrum is also created by something called epigenetics, which is a concept that has shown that training, diet, chemicals, or environment can effect your genes.(1) For example someone may have a genetic predisposition for heart disease but lifestyle choices can decrease or increase the likelihood of them ending up with heart disease.
When looking at hypermobility spectrum disorders we’ll start on the right hand side of the picture, underneath the umbrella of EDS. These individuals present with a lot of symptoms, such as persistent subluxations, multiple surgeries, pain, fatigue, anxiety, vascular, and GI issues. Now for most exercise professionals they will not be seeing these individuals in the gym, but I think its important to know the severity at which this condition can present.
As you move towards the left on the spectrum there are those diagnosed with EDS, but their symptoms are less severe, manageable, or have learned to be tolerated. Some are even high functioning and participating in high level activities. I often wonder if the intense training of some gymnasts and ballerinas from an early age does not have an epigenetic effect and possibly decrease the physical symptoms of this sometimes debilitating condition. Of course this is just a hypothesis for future researchers.
Moving along to the left we are now outside the umbrella of an EDS diagnosis. They have what is sometimes termed joint hypermobility syndrome. They present mostly with laxity but in the research they are found to still have some systemic symptoms. As I said, its a complex condition to deal with. These individuals I’ve found, seem to have figured out how to manage the symptoms fairly well and can be performing at high levels. They can be found in self selected activities where their flexibility serves as an asset such as ballet, gymnastics, yoga, acrobatics, or really any number of physical disciplines.
Working our way all the way to the left on the spectrum are the people that I wouldn’t consider inherently hypermobile, even though they may be a contortionist. You only need to ask these individuals one illuminating question, ‘Did you have to work hard for that full split?’ If they answer ‘Yes!’, they don’t have a genetic propensity for laxity in their tissue. They have persistently loaded their tissue to change its structure to serve their needs. They created extreme ranges in the joint, but it is not inherent. They will most likely have no other symptoms relating to deficits in collagenous structure.
TAKE HOME
Even amongst all of this variability the main common denominator is this joint laxity. So wherever they are on the spectrum you still have to contend with the idea that they have a whole lot of range in their joints. This range and joint laxity can create the “feeling” of swimming around in the joint as well as the symptom of not having great proprioception.
So main goals need to be start proximally at the joint and shore them up with strength and isolated movement work. Doing this you are able to strengthen as well as speak to the brain and gain increased proprioception. Practices like functional range conditioning(FRC), as well as resistance stretching, balance work, and perturbation type training are all good techniques to use to enhance the strength and stability of their joints.
Other key things to work on is creating tension and global strength to essentially cinch their bones together. Slow tempo work is key when doing strength work, they will often use speed to help them create movement because they have no bounce or resistance in their tissues itself to push off of. Moving slow also helps increase the proprioceptive ability, as well as get more time under tension. Win, win.
If you work with this population you have to be patient, and every person is individual. No one case will be like the next. Pain is another symptom that is highly prevalent so its a good idea to up on the latest pain science before working with this crowd. Like all chronic conditions, and really anybody, always take care of the low hanging fruit of sleep, stress, family, and nutrition before you tackle any other concerns.
1)Jorge Alejandro Alegría-Torres, Andrea Baccarelli, and Valentina Bollati, Epigenetics and lifestyle. Epigenomics. 2011 June ; 3(3): 267–277.
3 Responses
Thanks Cat! I work on people with hyper mobility in my practice and this really helps me to understand it better. You have provided a wide ranging consideration of the issues and I appreciate that.
Also, it would be interesting to hear an explanation of how the box of related conditions, like anxiety and panic disorder, are related. In particular I wonder if there is research on the correlation of joint laxity and anxiety. It makes sense.
I have a whole course on my website (fitwizesf.com) that explains all the physiology of the mysterious symptoms. There is quite a bit of research coming out about the connection with anxiety and hypermobility. Here’s a reference of one of the more recent articles. Mallory I-Bague Eur. Pshychiatry 2015 Jun;30(4):454-8. doi: 10.1016/j.eurpsy.2015.01.004. Epub 2015 Feb 13.
Glad you enjoyied it and found it useful.